Fibromyalgia is a disorder characterized by widespread musculoskeletal pain and sensitivity to touch along with fatigue, problems with sleep and memory and brain fog, People diagnosed with fibromyalgia also often suffer from anxiety, chronic fatigue, depression, irritable bowel syndrome, migraine and tension headaches, painful bladder disorder and TMJ (jaw pain).

According to the Mayo Clinic, “Fibromyalgia can’t be easily confirmed or ruled out through a simple laboratory test. You can’t detect it in your blood or see it on an X-ray. .Because there is no test for fibromyalgia, we must rely solely on your group of symptoms to make a diagnosis.”
However other blood tests can be taken to rule out conditions like auto -immune, thyroid dysfunction, anemia, viral or bacterial infection, nutritional deficiencies etc.
One of the first things I look at is the patient’s diet/lifestyle: are they eating processed foods, soda,etc.;drinking enough water; have a history of medications or antibiotics; are they taking the wrong supplements (too little- too much); do they have food allergies or intolerance?
It’s not a Food Allergy; maybe it’s a Food Intolerance
I would suspect a leaky gut syndrome and the need to change the person’s diet, test them for allergies/intolerance (igE/IgG) and ileo-cecal problems and the need for prebiotics and probiotics and other supplements to help repair their gut.
A NYC Applied Kinesiologist on Your Ileo-Cecal Valve (& Houston’s) & Your Health
The Correct Use of Muscle Testing in Nutritional Evaluation in Applied Kinesiology
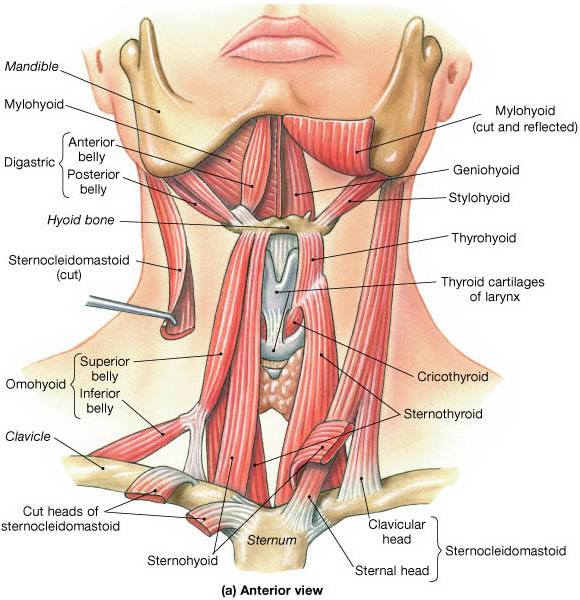
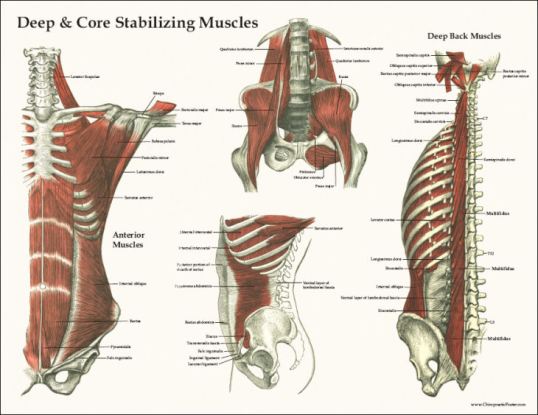
As a Applied Kinesiologist, I test for the function of individual muscles. Are they weak or strong.? The questions to be asked are: why is the muscle weak? Is the muscle on the other side hypertonic or “too stronger.”
As a NKT practitioner, I ask “Is there a dysfunction in the coordination of muscles working in patterns?” I would identify muscle imbalances by using muscle testing to determine what muscles are inhibited and what muscles are compensating (facilitating)for them.
Are these factors causing the muscles to be sensitive to touch?
Is there a problem with the vascular or lymphatic drainage of that muscle?
I might use neuro-lymphatic , neuro-vascular points and acu-points to increase lymphatic, blood and chi energy to organs and muscles.
How an Applied Kinesiologist Uses Neuro Lymphatics to Improve Health
How a NYC Applied Kinesiologist Uses Neurovascular Pts for Better Physical and Emotional Wellbeing.
Using AK techniques, the flow of energy in the meridians to the organs and muscles can be evaluated and corrected if out of balance. Correction can be made by many methods of stimulation, such as electrical, small tape patches with metal balls, or simply by mechanically stimulating certain spots. There is usually an immediate improvement in muscle/organ function after meridian balancing.
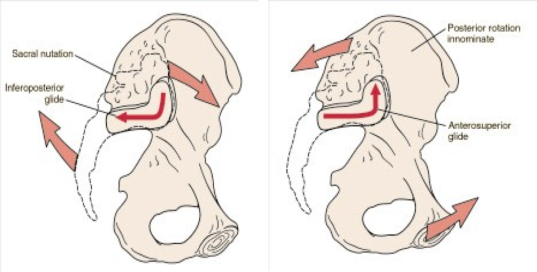
Is there a problem with the cranial-sacral system? The purpose of the movement of the cranial-sacral system is to aid the circulation of the cerebrospinal fluid throughout the central nervous system.
Some have suggested that CSF flow along the cranial nerves and spinal nerve roots allow it into the lymphatic channels. Restoring normal cranial-sacral rhythm enables the body to function optimally and may alleviate a wide variety of painful and dysfunctional conditions within the body.
Cranial Sacral Therapy in Applied Kinesiology
Is the patients under chronic stress? Can I help this patient w/ stimulation of their adrenals or with certain supplements?
Is the patient using their diaphragm correctly to order to get enough oxygen to their body? Stimulation of the diaphragm via spinal adustment and neuro-vasular/neuro-lymphatic/acu-points are done. Patient is taught how to use their diaphragm to get more oxygen into their system.
Can the patient tolerate gentle exercise like chi gong which is is a form of gentle exercise composed of movements that are repeated a number of times, often stretching the body, increasing fluid movement (blood, synovial and lymph) and building awareness of how the body moves through space.?
As a chiropractor, I can use non-force adjustments. It provides a gentle force into the spine of the patient through a very carefully directed and controlled pressure. This method is performed to be able to restore a stronger position and motion to fixated spinal joints taking pressure off the nerves exiting the spinal vertebrae which control the muscles and organs of the body.
These are some of the questions that need to addressed w/ the the complex problem of fibromyalgia; each patient is different and their needs must be addressed.
© 2018-Dr. Vittoria Repetto
Want more information on Dr. Vittoria Repetto and her NYC Applied Kinesiology/Chiropractic/ NKT practice at 230 W 13th St., NYC 10011; please go to www.drvittoriarepetto.com
And please check out the Patient Testimonials page on my web site.
Want to be in the know on holistic information and postings?
https://www.facebook.com/wvillagechiropracticappliedkinesiologynkt/
Or join me at Twitter: www.twitter.com/DrVRepetto