One of the major complaints that causes patients to seek out a doctor of chiropractic is low back pain; it can be caused by either a problem with the lumbar spine or the sacrum.
As a doctor of chiropractic who is also an applied kinesiologist, I use a technique developed by Dr. DeJarnette called Sacro Occipital Technique (SOT); so named because of the relationship between the sacrum (base of the spine) and the occiput (base of the skull).
One of the functions of the sacrum is to pump cerebro-spinal fluid (CSF) from the base of the spine back up the spinal canal to the brain and throughout the nervous system. The occiput also helps to pump CSF. The minute rhythmical motion is essential to optimal health – CSF effectively acts as the circulatory system of the brain and spinal cord.
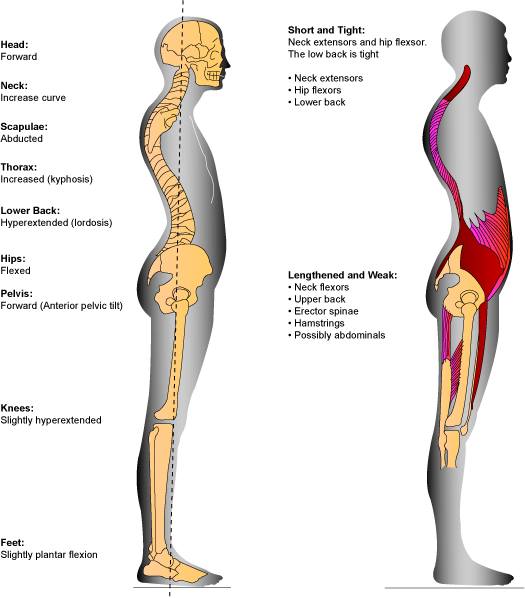
The pelvis forms the foundational support of the human skeleton. It supports the upper body right up to the skull, and enables us to transfer our weight to our legs. The sacrum is a large bone located at the terminal part of the vertebral spine, where it forms the posterior aspect of the pelvis. The spine holds our body upright, supports all of our organs and provides anchor points for our muscles. It also protects our delicate nervous system. The nervous system controls our body, and can only function normally when our structures are balanced and our pelvis, sacrum and lumbar is stable.
Dr. DeJarnette’s studied two aspects of the sacroiliac joint; the anterior synovial portion and the posterior hyaline cartilage portion. The anterior sacroiliac joint should have motion and this is where sacral nutation and counternutation takes place. The posterior sacroiliac joint is focused on weight-bearing stability and support, which is why at the posterior joint surface there are interlocking of the ridges, and grooves by structures like muscles, ligaments and fascia.
DeJarnette evaluated the weight-bearing characteristics of the sacroiliac joint and determined that when the joint could not adequately support body weight then load bearing stress will be moved upward to the L5/S1 and L4/5 discs, most commonly.
DeJarnette developed an analysis which classified pelvic problems into three different categories and three different non-force techniques using SOT blocks in positions that correct the involved category.

One of the major complaints that causes patients to seek out a doctor of chiropractic is low back pain; it can be caused by either a problem with the lumbar spine or the sacrum.
As a doctor of chiropractic who is also an applied kinesiologist, I use a technique developed by Dr. DeJarnette called Sacro Occipital Technique (SOT); so named because of the relationship between the sacrum (base of the spine) and the occiput (base of the skull).
One of the functions of the sacrum is to pump Cerebro-Spinal Fluid (CSF) from the base of the spine back up the spinal canal to the brain and throughout the nervous system. The occiput also helps to pump CSF. The minute rhythmical motion is essential to optimal health – CSF effectively acts as the circulatory system of the brain and spinal cord.
Dr. DeJarnette’s studied two aspects of the sacroiliac joint; the anterior synovial portion and the posterior hyaline cartilage portion. The anterior sacroiliac joint should have motion and this is where sacral nutation and counternutation takes place.


The posterior sacroiliac joint is focused on weight-bearing stability and support, which is why at the posterior joint surface there are interlocking of the ridges, and grooves by structures like muscles, ligaments and fascia.

DeJarnette evaluated the weight-bearing characteristics of the sacroiliac joint and determined that when the joint could not adequately support body weight then load bearing stress will be moved upward to the L5/S1 and L4/5 discs, most commonly.
DeJarnette developed an analysis which classified pelvic problems into three different categories and three different non-force techniques using SOT blocks in positions that correct the involved category.
Category One is a pelvic torsion with altered sacral nutation(motion) This lack of nutation affects the spinal and cranial meningeal and CSF systems which function to a degree like a closed kinematic chain. Therefore symptoms can be low back pain, chronic shoulder complaints, thoracic outlet syndrome, CSF stagnation, and altered vasomotor function.
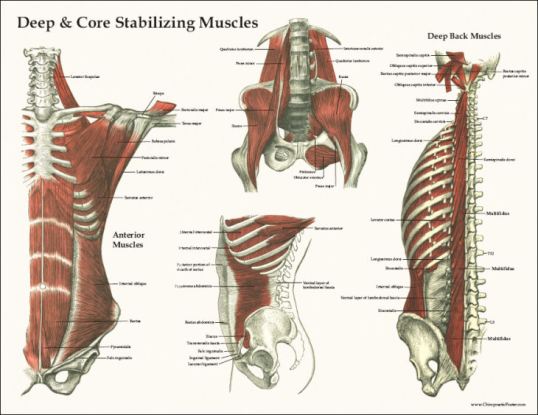
Involved muscles can be the piriformis, quadratus lumborum, sacrospinalis, gluteus medius and gluteus maximus. As an applied kinesiologist, I’d check to see if they are hypotonic or hypertonic; as a neurokinetic therapist, I’d check to see if a muscle is weak (or inhibited) by another muscle compensating.
Therapy localization (TL) is done by putting 2 hands on each sacral-iliac joint and then challenging the pelvis for a structural listing and then blocks are put under the patient’s pelvis based to the findings.
The positive Tl’ed side is not adjusted. Cranials are checked.
Category Two happens when ligaments that hold the sacroiliac joint are stretched or sprained, allowing the joint surfaces to separate. Stress can aggravate this ligament weakness via adrenal hormone overdrive.
Symptoms can be low back pain, bowel complaints, possible dysfunction of the reproductive glands and the adrenals, shoulder problems and decreased cervical range of motion.
Involved muscles in addition to the ones mentioned in Category I are the sartorius, gracilis, rectus abdominals and hamstrings along with the iliolumbar ligament. These structures are tested via applied kinesiology and neurokinetic protocols mentioned above. Cranials again are checked.
Category Three occurs when the low back can no longer tolerate the physical stressors placed on it and involves both disc and nerve root aggravation. This can be a sudden one-off event such as a lift, or it can be a pre-existing weakness that is aggravated. Often Category Three produces pain in the low back and sometimes pain radiates down a leg as sciatica.
Muscles to be checked are the psoas as it attaches into the front of the lumbar vertebrae as well as the muscles involved in Category One as Category Three can be a Category One that was never corrected.
Correction in all the categories involves using blocks under the pelvis in specific directions related to the category and the subluxation/misalignment of the pelvis/sacrum. The patient’s weight and breathing help to balance the low back, sacrum and CSF flow and takes the pressure or irritation off the nerve. This allows the body to heal.
Patient is told to ice the involved areas, how to do daily activities, given stretches and exercises and advised on nutrition to help the body heal.
For more information on issues mentioned:
Cranial Sacral Therapy in Applied Kinesiology
How a Combination of Applied Kinesiology, NeuroKinetic Therapy and Chiropractic Works
The Use of Applied Kinesiology in a Chiropractic Examination
© 2017-Dr. Vittoria Repetto
Want more information on Dr. Vittoria Repetto and her NYC Applied Kinesiology/Chiropractic/ NKT practice at 230 W 13th St., NYC 10011; please go to www.drvittoriarepetto.com
And please check out the Patient Testimonials page on my web site.
Want to be in the know on holistic information and postings?
https://www.facebook.com/wvillagechiropracticappliedkinesiologynkt/
Or join me at Twitter: www.twitter.com/DrVRepetto